If you are reading this because you or someone you love has noticed a sore in the mouth that will not heal, or a white patch that appeared without any obvious reason — you are right to look into it. Most mouth lesions are completely harmless. But some need attention, and knowing the difference matters.
I see patients every week who waited too long before coming in, not because they were careless, but because the early signs of oral cancer are easy to dismiss. A small ulcer. A slightly numb patch. Nothing that feels alarming on a busy day. This page is meant to help you look at those signs more carefully — and decide clearly when it is time to speak to a specialist.
| Quick Fact | What You Should Know |
| Most common type | Squamous cell carcinoma (SCC) – affects the lining of the mouth and throat |
| Most affected sites | Tongue (lateral border), inner cheek (buccal mucosa), floor of mouth, gingiva |
| Leading risk factor in India | Tobacco chewing, betel nut (areca nut), and gutka use |
| Age group most affected | Usually 40 years and above; increasingly seen in younger patients |
| Early detection impact | Stage I oral cancer: 5-year survival often exceeds 80% |
| Stage IV survival | Significantly lower — reinforcing why early evaluation matters |
| First step if concerned | See an Oral & Maxillofacial Surgeon for clinical examination |
| NCCN Guideline | NCCN Head and Neck Cancers Guidelines recommend biopsy for any suspicious oral lesion persisting beyond 2–3 weeks |
Oral Cancer Symptoms Oral cancer most commonly appears as a mouth ulcer that does not heal within three weeks, a white or red patch inside the mouth, a painless lump in the neck, or difficulty swallowing. Key risk factors include tobacco use (smoked and smokeless), alcohol, and areca nut (betel nut) consumption. Early detection significantly improves the outcome of treatment.
What Is Oral Cancer?
Oral cancer refers to cancer that develops in any part of the oral cavity — the lips, tongue, gums, the lining of the cheeks (called the buccal mucosa), the roof of the mouth (hard palate), the floor of the mouth beneath the tongue, and the area behind the last molars (retromolar trigone).
The large majority of these cancers — roughly 90% — are a type called squamous cell carcinoma (SCC). This means the cancer arises from the flat, skin-like cells that line the inside of the mouth. The remaining 10% include less common types such as salivary gland tumours and mucosal melanoma.
In India, oral cancer is one of the most common cancers overall, and it carries a particular burden in states like Tamil Nadu, where tobacco and areca nut use are culturally prevalent. At Apollo Hospitals in Chennai, a significant proportion of the patients I see have had symptoms for months before seeking an opinion — which is precisely why public awareness of the early signs matters so much.
Common Sites in the Mouth
Cancer does not arise randomly. Certain parts of the mouth are more vulnerable than others, typically because of sustained carcinogen exposure from tobacco or areca nut.
| Site | Clinical Notes |
| Lateral border of tongue | Most common site globally; often painless in early stages |
| Buccal mucosa (inner cheek) | Most common site in India due to tobacco/areca nut chewing habits |
| Floor of the mouth | High-risk site; close proximity to floor tissues can delay detection |
| Gingiva (gum tissue) | Often confused with dental infection or tooth-related pain |
| Hard palate | Less common; may appear as a firm swelling or non-healing ulcer |
| Retromolar trigone | Area behind last molar; often detected late due to limited visibility |
| Lip (vermilion border) | More common in fair-skinned individuals with prolonged sun exposure |
The Role of a Maxillofacial Surgeon in Early Detection
When a mouth lesion looks clinically suspicious, an Oral & Maxillofacial Surgeon is the appropriate specialist to assess it. Dentists are a valuable first point of contact, but a formal evaluation, biopsy, and treatment planning require specialist input.
Early Warning Signs: What to Look For
The challenge with oral cancer is that its earliest signs are easy to normalise. A small ulcer, a slightly rough patch of tissue, a vague ache that comes and goes. None of these feel dramatic. But there are specific features that separate a common, benign mouth sore from something that warrants a closer look.
Non-Healing Ulcers and Persistent Patches
A mouth ulcer that has not healed after three weeks is the most important warning sign. Normal ulcers — whether from a bitten cheek, a sharp food fragment, or stress-related canker sores — heal within one to two weeks. If yours has not, that timeline alone is a reason to seek an opinion.
White patches that cannot be wiped off are called leukoplakia. Red, velvety patches are called erythroplakia. Both are considered potentially pre-malignant — meaning they may, in some cases, progress to cancer if left untreated.
Erythroplakia carries a significantly higher risk of malignant change than leukoplakia — transformation rates range from 14% to 50% in published literature, and nearly half of lesions already show carcinoma on first biopsy. All erythroplakic lesions should be biopsied without delay.
In patients who chew tobacco or areca nut, a specific condition called Oral Submucous Fibrosis (OSMF) is common. This causes progressive stiffening of the mouth, reduced mouth opening, and a burning sensation. It is considered a high-risk pre-malignant condition in the Indian population.
Unusual Bleeding, Numbness, or Lumps
A lesion that bleeds easily when touched by the tongue or food — without any obvious reason like a sharp tooth or denture injury — is worth evaluating. Similarly, a persistent patch of numbness or tingling in the lip, chin, or cheek may suggest nerve involvement by an underlying tumour.
A painless lump in the neck that has appeared over a few weeks is one of the most significant signs that lymph nodes may be involved. Lymph nodes (small glands in the neck that are part of the immune system) often enlarge when cancer has begun to spread from the primary site in the mouth. A firm, non-tender neck lump alongside any oral symptom should prompt an urgent review.
Difficulty Swallowing, Speaking, or Opening the Mouth
As a lesion grows, it may begin to interfere with function. Difficulty swallowing (called dysphagia), a change in the quality of the voice, restricted tongue movement, or reduced mouth opening (called trismus) are all signs of more advanced local disease. These symptoms suggest that the tumour may have grown into adjacent muscle, bone, or deeper tissue.
Summary: Warning Signs That Need Evaluation
- Mouth ulcer or sore present for more than 3 weeks
- White patch (leukoplakia) or red patch (erythroplakia) that will not go away
- Lesion that bleeds easily on contact
- Firm or hard feeling at the base of an ulcer (induration)
- New painless lump in the neck
- Numbness or tingling in the lip, cheek, or chin
- Difficulty swallowing, speaking, or fully opening the mouth
- Loosening of a tooth near the lesion with no dental explanation
Burning sensation and reduced mouth opening (if chewing tobacco or areca nut)
Understanding the Causes and Risk Factors
Oral cancer does not have a single cause. In most cases, it develops when the cells lining the mouth accumulate enough genetic damage — over months or years — to begin growing in an uncontrolled way. Several well-established factors accelerate this process.
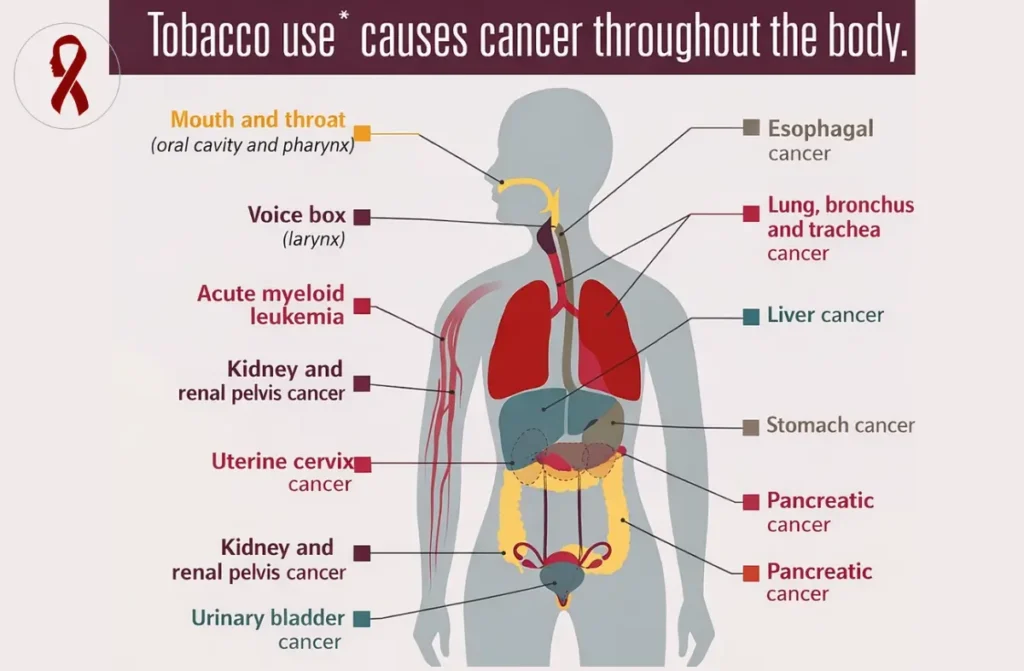
Tobacco — Smoked and Smokeless
Tobacco is the single most important risk factor for oral cancer in India. This includes cigarettes, beedis, hookah, and cigars — but also smokeless forms such as gutka, khaini, mishri, and pan masala. Smokeless tobacco is particularly relevant in Tamil Nadu and across South Asia, where it is often chewed throughout the day.
The carcinogens in tobacco — including nitrosamines and polycyclic aromatic hydrocarbons — damage the DNA of mucosal cells with repeated exposure. The risk is dose-dependent and duration-dependent: the longer and more heavily someone uses tobacco, the higher their risk. Importantly, the risk does not disappear immediately on quitting, though it does reduce significantly over time.
Betel Nut and Areca Nut Use
This is a risk factor that deserves specific attention for patients in Chennai and across South and Southeast Asia. The areca nut — commonly chewed with betel leaf, slaked lime, and often tobacco — is independently carcinogenic. Even areca nut preparations without tobacco (such as plain supari) carry a measurable cancer risk.
Areca nut is the primary driver of Oral Submucous Fibrosis (OSMF), a condition that causes progressive mucosal fibrosis — the internal tissue of the mouth becomes scarred and stiff. OSMF is considered a high-risk pre-malignant condition, and patients with this diagnosis need regular surveillance. Globally, India has among the highest rates of OSMF and areca nut-related oral cancer.
Alcohol
Alcohol is an independent risk factor for oral cancer, and its effect is significantly amplified when combined with tobacco use. The combination of heavy tobacco use and heavy alcohol consumption is associated with a substantially higher risk than either factor alone. Alcohol may act as a solvent that increases mucosal permeability to carcinogens, while also having its own direct mucosal effects.
Human Papillomavirus (HPV)
HPV — particularly HPV-16 — is now recognised as a significant cause of oropharyngeal cancers (cancers of the tonsil and base of tongue). Its role in true oral cavity cancer is smaller but not negligible. HPV-related head and neck cancers tend to occur in younger, non-smoking patients and generally carry a better prognosis than tobacco-related cancers when treated appropriately.
In clinical practice in Chennai, the majority of oral cavity cancers I see are tobacco- and areca nut-related rather than HPV-driven. HPV testing is now included in pathology assessment for oropharyngeal primaries, as it has both prognostic and treatment-planning implications.
Other Contributing Factors
Prolonged sun exposure increases the risk of lip cancer specifically. Poor oral hygiene and chronic dental trauma — from a sharp tooth edge or an ill-fitting denture — may contribute to sustained mucosal irritation, though these are considered minor risk factors relative to tobacco and areca nut. Immunosuppression, including HIV infection, is associated with elevated oral cancer risk.
Risk: What Patients From High-Risk Groups Should Know
If you chew tobacco, areca nut, or gutka — please arrange a mouth screening with your dentist or an Oral & Maxillofacial Surgeon every 6–12 months, even if you have no symptoms. Early-stage lesions in these patients are often subtle and entirely asymptomatic. Stopping tobacco and areca nut use remains the single most important thing you can do to reduce your risk.
When Should You See an Oral Cancer Specialist?
The threshold is straightforward: if you have a mouth sore, patch, or swelling that has been present for three weeks without improvement, book an appointment. You do not need to wait for a referral. You can contact an Oral & Maxillofacial Surgeon directly.
See a Specialist If You Have Any of the Following
- A mouth ulcer or sore lasting more than 3 weeks
- A white or red patch inside the mouth that appeared without an obvious cause
- A painless lump in the neck, particularly if it appeared over a few weeks
- Bleeding from a mouth lesion on gentle contact
- Numbness of the lip, cheek, or chin without a dental explanation
- Restricted mouth opening or difficulty swallowing — especially in tobacco users
- A tooth extraction site that has not healed after 4–6 weeks
- Any concern in a patient with known OSMF or a history of leukoplakia
You can reach me at Apollo Hospitals, Greams Road, Chennai. A clinical assessment does not commit you to any treatment — it gives you information.
About the Author
Dr. Pradeep S., MDS
Oral & Maxillofacial Surgeon | Fellow – Head & Neck Oncology
Apollo Hospitals, Chennai
Dr. Pradeep S. is an Oral & Maxillofacial Surgeon practicing at Apollo Hospitals, Chennai, with a special interest in oral cancer surgery and head & neck oncology. He evaluates and treats patients with cancers of the tongue, buccal mucosa, gingivobuccal complex, and other oral cavity sites, as well as precancerous oral conditions.
His clinical work includes oncologic resection of oral tumors, neck dissection for lymph node involvement, and multidisciplinary management of oral cancer in collaboration with oncology, radiation therapy, and reconstructive surgery teams.
Dr. Pradeep is actively involved in oral cancer awareness, early detection initiatives, and patient education, with a focus on promoting early diagnosis and improving treatment outcomes.
Clinical Focus
- Oral cancer diagnosis and surgical management
- Tongue cancer and buccal mucosa cancer
- Neck dissection for oral cancer
- Management of oral potentially malignant disorders
- Early detection and screening of oral cancer
Hospital Affiliation
Apollo Hospitals, Chennai
Medical Review
This article has been medically reviewed for clinical accuracy by Dr. Pradeep S., Oral & Maxillofacial Surgeon at Apollo Hospitals, Chennai.
Last medical review: March 2026
Medical Disclaimer
This article is intended for general patient education and does not constitute medical advice. The information provided is not a substitute for a clinical evaluation by a qualified surgeon or physician. If you have concerns about a mouth ulcer or any oral symptom, please seek an in-person assessment from an appropriately trained clinician.